While PD-L1 testing is widely used to guide immunotherapy decisions, a low or negative PD-L1 result does not necessarily mean immunotherapy will not work. Clinical studies have shown that some patients with low PD-L1 expression still benefit from immune checkpoint inhibitors, particularly when immunotherapy is combined with chemotherapy or used in specific clinical settings. This reflects the complexity of tumor-immune interactions and highlights the broader role of precision oncology beyond a single biomarker.
In modern oncology practice, PD-L1 expression is one component of a larger biomarker framework. Treatment decisions increasingly integrate molecular profiling, tumor biology, and clinical context.
Clinical perspective: Biomarkers guide therapy, but no single marker completely predicts response to immunotherapy.
Why PD-L1 Alone Does Not Fully Predict Immunotherapy Response
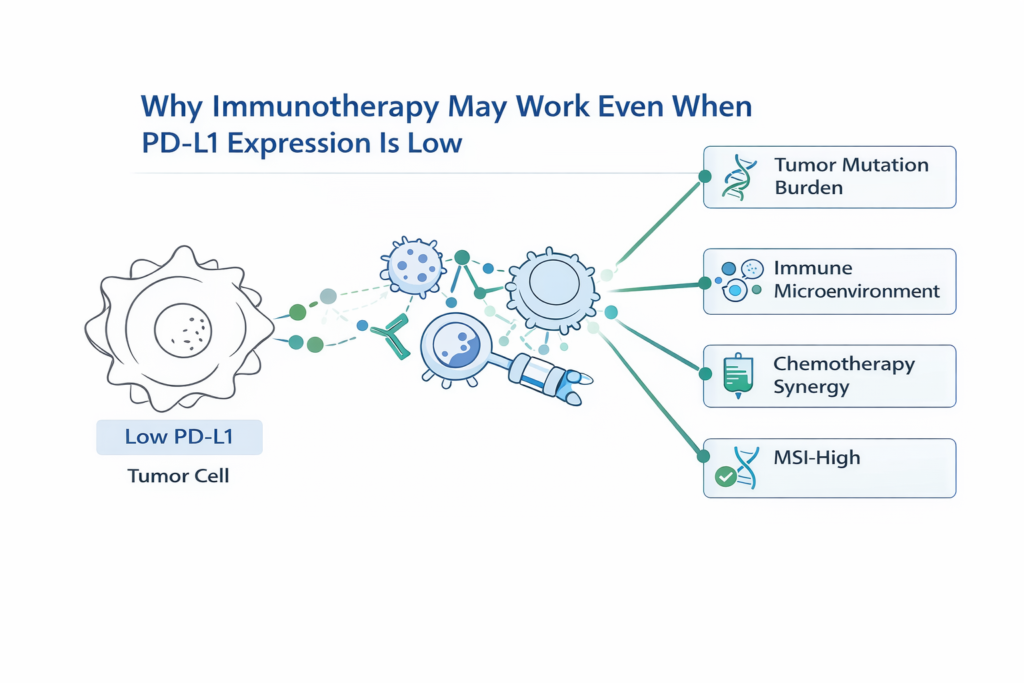
PD-L1 expression reflects one aspect of the tumor immune environment, but cancer-immune interactions are far more complex.
- Tumor mutation burden
- Presence of tumor-infiltrating lymphocytes
- Genomic instability
- Neoantigen load
- Immune microenvironment signaling
These biological factors can influence whether a tumor responds to immunotherapy even when PD-L1 levels appear low.
In Which Situations Can Immunotherapy Work With Low PD-L1?
Clinical trials and real-world oncology practice have demonstrated meaningful responses in certain situations.
- Immunotherapy combined with chemotherapy
- High tumor mutation burden
- Microsatellite instability-high (MSI-H) tumors
- Immune-active tumor microenvironment
- Specific tumor types where PD-L1 is less predictive
In these contexts, the immune system may still be capable of mounting an anti-tumor response once immune checkpoints are blocked.
Understanding Combination Immunotherapy Strategies
Combination therapy can enhance the effectiveness of immunotherapy even in tumors with low PD-L1 expression.
- Chemotherapy can increase tumor antigen release.
- Immune priming can activate anti-tumor immune cells.
- Checkpoint inhibitors then amplify immune response.
This strategy is commonly used in several cancers including lung cancer, where immunotherapy plus chemotherapy improves outcomes compared with chemotherapy alone.
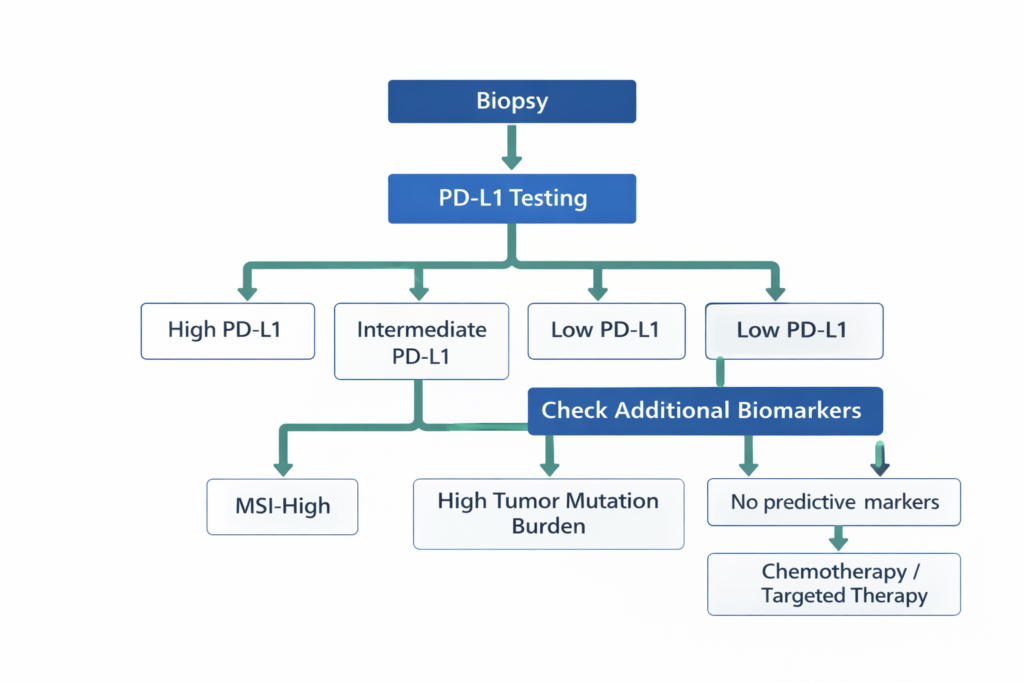
Clinical Decision Logic
- If PD-L1 is high → Immunotherapy may be used as monotherapy.
- If PD-L1 is intermediate → Combination immunotherapy strategies are often considered.
- If PD-L1 is low → Immunotherapy may still be effective when combined with chemotherapy.
- If MSI-H or high tumor mutation burden → Immunotherapy may still provide strong benefit.
- If actionable mutation exists → Targeted therapy may take priority.
Why Comprehensive Biomarker Testing Matters
PD-L1 results should always be interpreted alongside broader molecular testing.
- Next-generation sequencing (NGS)
- Tumor mutation burden
- Microsatellite instability testing
- Driver mutation analysis
A comprehensive molecular evaluation ensures that treatment strategy reflects the full biological profile of the tumor rather than relying on a single biomarker.
Frequently Asked Questions
If PD-L1 is negative, should immunotherapy be avoided?
No. Immunotherapy can still be beneficial depending on tumor biology and treatment strategy.
Why do some PD-L1 negative patients respond to immunotherapy?
Other biological mechanisms such as tumor mutation burden and immune cell infiltration may drive response.
Does chemotherapy help immunotherapy work better?
Yes. Chemotherapy can increase tumor antigen release and enhance immune activation.
Is PD-L1 testing still important?
Yes. PD-L1 remains a valuable biomarker for treatment stratification.
Should biomarker results be reviewed before treatment?
A structured review of pathology and molecular reports can help optimize treatment selection.
Related Articles
The Role of PD-L1 Testing Before Starting Immunotherapy
What Is Biomarker-Driven Therapy in Modern Oncology?
Review of low PDL1 in solid cancers – ASCO
Closing Perspective
Immunotherapy has transformed cancer treatment, but predicting response remains complex. PD-L1 testing offers valuable guidance, yet it represents only one component of a broader precision oncology strategy.
Integrating molecular profiling, immune biomarkers, and clinical context allows oncologists to personalize treatment decisions with greater precision.
Educational Disclaimer
This article is intended for educational purposes and should not replace individualized medical advice. Treatment decisions should always be made in consultation with a qualified oncology specialist.
Pingback: Role of PD-L1 testing before immunotherapy