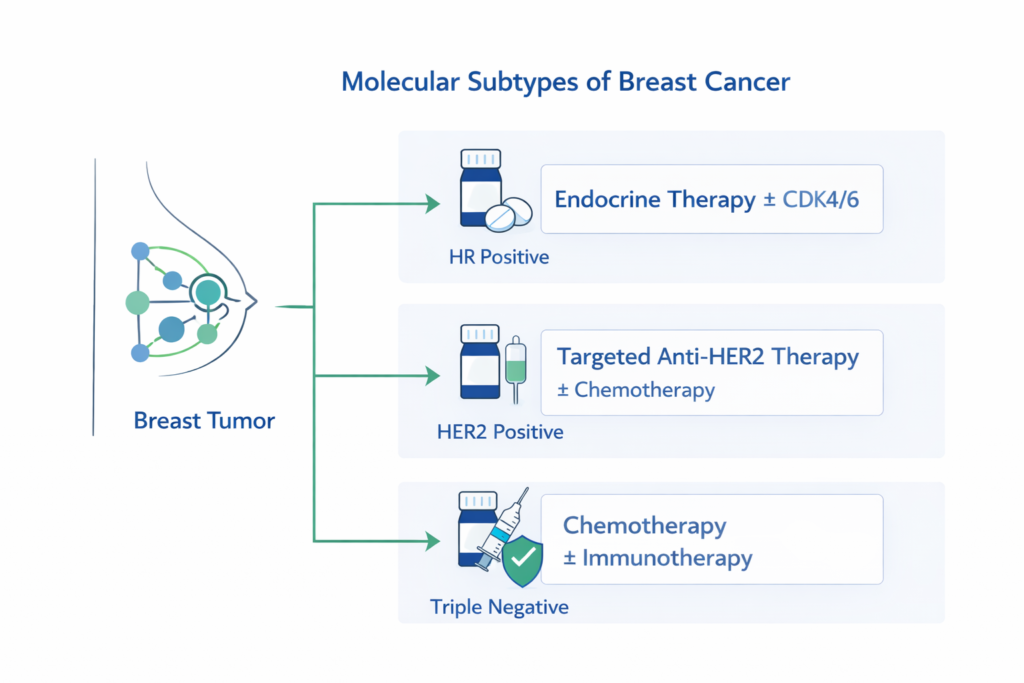
Molecular subtypes of Breast cancer is biologically classified using ER, PR, and HER2 status (and sometimes proliferation/genomic assays). These markers define clinically meaningful subtypes—HR-positive, HER2-positive, and triple-negative—which directly determine the backbone of treatment (endocrine therapy, anti-HER2 therapy, chemotherapy, and selected immunotherapy).
In breast oncology, accurate receptor profiling is not an optional detail—it is the starting point for evidence-based sequencing and avoiding under- or overtreatment.
Which Markers Define Breast Cancer Molecular Subtypes?
Routine classification uses immunohistochemistry (IHC) for ER/PR and HER2 assessment (IHC ± ISH for confirmation when needed). These results map to treatment-sensitive subgroups.
- HR-positive: ER and/or PR positive
- HER2-positive: HER2 overexpression or amplification
- Triple-negative: ER negative, PR negative, HER2 negative
Additional tools (e.g., Ki-67 and genomic assays in selected early-stage HR-positive disease) may refine prognosis and chemotherapy benefit, but do not replace core receptor profiling.
How Does HR-Positive Disease Change Treatment Planning?
HR-positive tumors are driven by hormone signaling. Endocrine therapy is the backbone across early and advanced settings, with targeted agents added based on stage and risk.
- Primary backbone: endocrine therapy
- Advanced disease: endocrine therapy ± CDK4/6 inhibitors (common evidence-based approach)
- Early disease: chemotherapy decisions may be refined using clinicopathologic risk and selected genomic assays
What Is Unique About HER2-Positive Breast Cancer?
HER2-positive disease is highly targetable. Anti-HER2 therapy—often combined with chemotherapy depending on stage—has substantially improved outcomes in both early and metastatic settings.
- Key concept: HER2 targeting is essential when HER2 is truly positive
- Borderline/equivocal results require confirmatory testing and careful pathology correlation
How Is Triple-Negative Breast Cancer Typically Treated?
Triple-negative breast cancer (TNBC) lacks ER/PR/HER2 targets, so systemic therapy commonly relies on chemotherapy. Immunotherapy is considered in defined clinical contexts, particularly in selected advanced disease based on immune biomarkers.
- Mainstay: chemotherapy
- Selected cases: immunotherapy based on biomarker context and guideline-based eligibility
- Consider hereditary risk assessment in appropriate patients (e.g., young age/family history)
Subtype-to-Treatment Decision Tree
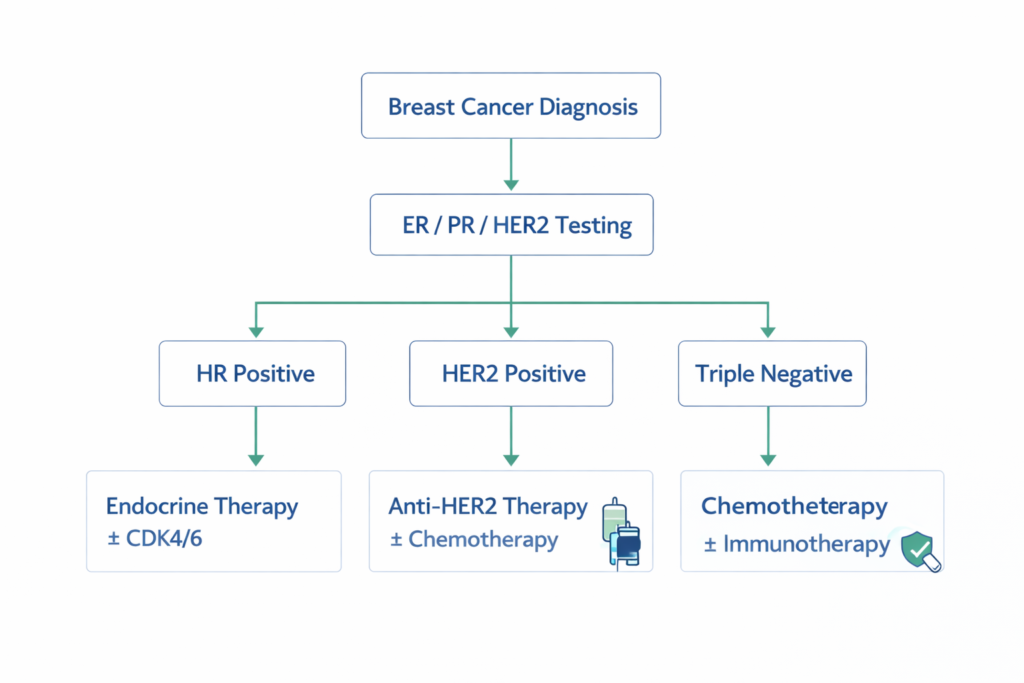
Decision Logic (If → Then):
- If HR positive → Then endocrine therapy forms the backbone (± targeted agents by stage/risk).
- If HER2 positive → Then add anti-HER2 therapy (± chemotherapy by stage/intent).
- If triple-negative → Then chemotherapy is primary; consider immunotherapy only when biomarker/clinical criteria support it.
Beyond subtype, final treatment sequencing depends on stage, nodal status, tumor burden, patient fitness, comorbidities, and intent (curative vs metastatic control).
When Is a Second Opinion Clinically Useful in Subtype-Based Planning?
A second opinion is most valuable when key determinants are uncertain or when sequencing choices carry major long-term impact.
- Equivocal HER2 (IHC 2+) needing ISH correlation
- Discordant receptor results across biopsy/surgery or between labs
- Neoadjuvant strategy decisions in stage II–III disease
- Younger patients where fertility preservation intersects with systemic therapy timing
Frequently Asked Questions
Can the breast cancer subtype change over time?
Yes. In metastatic disease, receptor status can evolve; re-biopsy may be considered when results would change treatment.
Do all HR-positive patients require chemotherapy?
No. Many HR-positive patients can be managed with endocrine-based strategies; chemotherapy decisions depend on clinical risk and selected genomic/biologic factors.
What should patients know about “borderline” HER2 results?
Borderline HER2 requires careful interpretation (IHC/ISH standards, pre-analytic factors, and pathology correlation). Treatment should be based on confirmed HER2 status.
Is triple-negative breast cancer always aggressive?
TNBC often has higher-grade biology, but outcomes vary by stage and treatment response. Early diagnosis and appropriate systemic therapy remain central.
Should BRCA testing be considered in triple-negative breast cancer?
Often yes, particularly in younger patients or those with suggestive family history, as results can influence risk management and selected therapy choices.
Related Articles
- Genetic Testing in Breast Cancer: When and Why It Matters
- Biomarker-Driven Therapy in Modern Oncology
- Structured Second Opinions in Cancer Care
Closing Perspective
Molecular subtyping has shifted breast oncology from “one-size-fits-all” to biology-led strategy. Accurate ER/PR/HER2 assessment is the anchor that informs therapy selection, sequencing, and intensity. The most durable outcomes come from aligning subtype biology with evidence-based treatment pathways.
Educational Disclaimer: This article is for educational purposes only and does not replace individualized medical advice, pathology review, or treatment planning with your oncology team.