Cancer treatment should not be determined by age alone. Elderly patients require physiologic assessment beyond chronological age, while adolescents and young adults (AYA) require biologically precise and survivorship-focused strategies. Individualization is achieved through structured evaluation of fitness, tumor biology, long-term risk, and life-stage priorities. Modern oncology integrates geriatric assessment and precision medicine to avoid both undertreatment and overtreatment.
In my clinical practice, age-specific oncology demands disciplined risk stratification rather than assumptions. A 78-year-old may tolerate therapy better than a 55-year-old with frailty. Similarly, a 28-year-old requires survivorship planning that extends decades beyond initial cure.
Why Is Chronological Age an Inadequate Treatment Determinant?
Chronological age does not equal biological age. Elderly patients vary widely in organ reserve, cognition, mobility, and social support.
- Renal clearance may differ significantly among patients of similar age.
- Cardiac reserve influences anthracycline or HER2-directed therapy decisions.
- Polypharmacy increases interaction risk.
- Functional independence predicts tolerance more than age itself.
Similarly, young adults face long-term toxicity considerations that older patients may not encounter.
How Should Cancer Treatment Be Structured in the Elderly?
Geriatric oncology relies on structured Comprehensive Geriatric Assessment (CGA).
- Functional status (ADL / IADL)
- Cognitive screening
- Comorbidity index
- Nutritional assessment
- Medication review
- Frailty scoring
This framework allows classification into:
- Fit: Eligible for standard therapy.
- Vulnerable: Modified dosing or schedule.
- Frail: Palliative-intent or low-intensity strategy.
The objective is precision in intensity selection.
What Makes AYA Oncology Clinically Distinct?
AYA oncology (ages 15–39) lies between pediatric and adult oncology frameworks.
- Unique tumor biology (e.g., certain sarcomas, germ cell tumors).
- Higher incidence of hereditary predisposition.
- Fertility preservation considerations.
- Psychosocial and career impact.
- Long-term survivorship risk.
For AYA patients, therapy must balance cure probability with decades of survivorship risk.
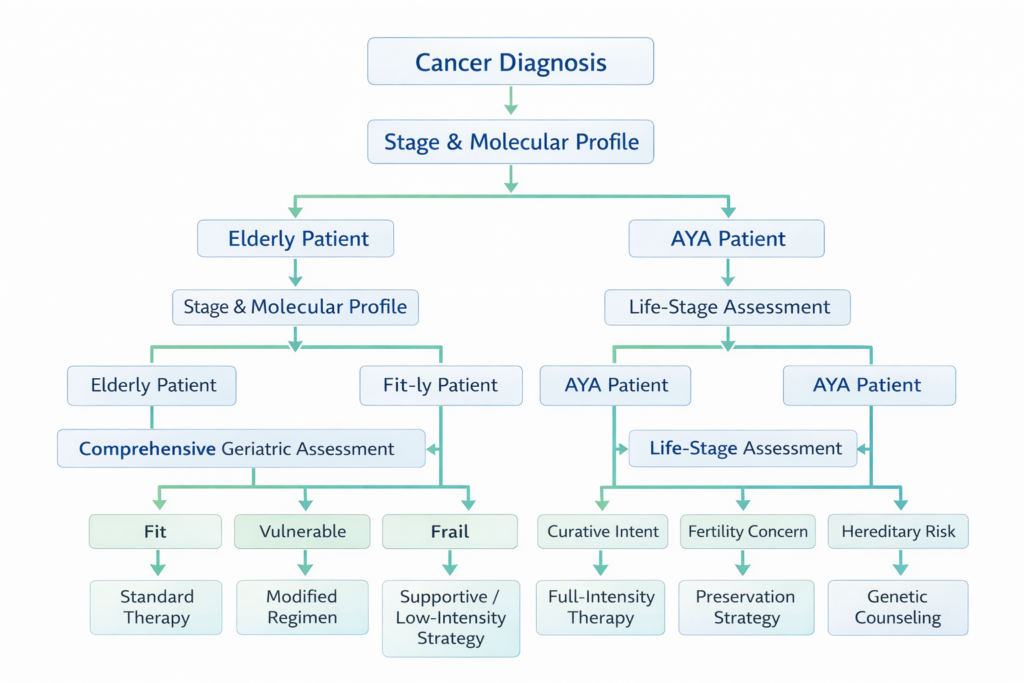
Structured Decision Logic: Age-Specific Treatment Planning
Step 1: Confirm stage and tumor biology.
Step 2: Assess age-specific risk framework.
- If elderly + fit → Standard guideline-concordant therapy.
- If elderly + vulnerable → Dose-adjusted or sequential regimen.
- If elderly + frail → Symptom-focused strategy.
- If AYA + curative intent → Maximize cure probability.
- If AYA + fertility concern → Integrate preservation strategy.
- If AYA + hereditary suspicion → Recommend genetic counseling.
This structured pathway prevents age-based bias and ensures biologically aligned decisions.
What Are the Risks of Undertreatment and Overtreatment?
Undertreatment in elderly:
- Assuming age equals intolerance.
- Withholding curative therapy unnecessarily.
Overtreatment in elderly:
- Ignoring frailty markers.
- Excess toxicity leading to hospitalization.
Overtreatment in AYA:
- Long-term cardiac or fertility harm.
- Secondary malignancy risk.
Balanced personalization mitigates these risks.
When Should a Structured Second Opinion Be Considered?
A second opinion becomes particularly relevant when:
- An elderly patient is denied standard therapy solely based on age.
- An AYA patient has not received fertility counseling.
- Genetic testing has not been evaluated in young onset cancers.
- Complex comorbidities complicate chemotherapy selection.
Frequently Asked Questions
Can elderly patients safely receive chemotherapy?
Yes, if physiologically fit. Dose modifications and careful monitoring are key.
What defines frailty in oncology?
Frailty includes reduced mobility, cognitive decline, malnutrition, and decreased physiologic reserve.
Why is fertility counseling important in AYA oncology?
Many cancer therapies impair reproductive function. Early discussion enables preservation options.
Are outcomes worse in elderly cancer patients?
Outcomes depend on fitness and biology rather than age alone.
Should genetic testing be routine in young cancer patients?
Young-onset cancers warrant evaluation for hereditary syndromes in many cases.
Related Articles
• Hereditary Cancer Syndromes in Young Adults
• Molecular Profiling in Advanced Cancers
• Structured Cancer Second Opinions
Closing Perspective
Geriatric and AYA oncology represent two ends of the age spectrum where personalization is not optional but essential. Treatment must integrate tumor biology, physiologic reserve, and life-stage implications. The discipline lies in structured assessment rather than chronological bias.
Educational Disclaimer: This article is intended for educational purposes only and does not replace individualized medical consultation. Treatment decisions must be made after comprehensive clinical evaluation.