Direct answer: Precision oncology is an approach to cancer treatment where the oncologist studies the cancer’s biology, biomarkers, molecular profile and the patient’s clinical condition before choosing treatment. In simple terms, it helps move beyond a “one-size-fits-all” cancer plan and supports more informed decisions about chemotherapy, targeted therapy, immunotherapy, clinical trials, genetic counselling and follow-up. Precision oncology cancer treatment is most useful when test results can meaningfully change treatment choice, sequencing or family-risk assessment.
This article belongs to the Precision Oncology & Molecular Medicine pillar.
Authority perspective: Written from the clinical perspective of Dr Raman Narang, Consultant Medical Oncologist in Delhi, with a focus on precision oncology, biomarker-guided treatment, cancer genetics and structured cancer second opinions.
Precision oncology is often misunderstood as simply “doing an NGS test” or “finding a targeted therapy.” In real practice, it is broader than that.
It starts with confirming the diagnosis, stage, pathology, fitness of the patient and treatment goal. Then, where appropriate, molecular testing, biomarker testing, genetic counselling or tumour board review may help refine the treatment plan.
For patients and families, the main question is not just “Which test should we do?” The better question is: “Will this information change the treatment decision?”
Who needs to understand precision oncology cancer treatment?
Precision oncology is relevant for many cancer patients, but it is not required in the same way for every diagnosis.
It is especially important when treatment decisions depend on cancer subtype, stage, biomarkers or molecular alterations. This is common in several advanced cancers, recurrent cancers and cancers where targeted therapy or immunotherapy may be considered.
Patients may need this discussion if they have lung cancer, breast cancer, ovarian cancer, colorectal cancer, prostate cancer, lymphoma, myeloma, leukemia or rare cancers where pathology and molecular features influence treatment.
Referring doctors may also find precision oncology useful when deciding when to send tissue for testing, when to refer for medical oncology review and when a second opinion may clarify the treatment sequence.
How does precision oncology actually help in cancer treatment?
Precision oncology helps by adding biological information to standard clinical decision-making. The oncologist still considers the cancer type, stage, symptoms, organ function and patient fitness. Biomarker and molecular information are then interpreted in that context.
In some patients, this may identify a targeted therapy. In others, it may support immunotherapy selection, avoid unnecessary treatment, suggest a clinical trial or explain why a standard treatment remains the most appropriate choice.
It can also help distinguish between treatment options when the same cancer has different biological subtypes. For example, two patients may both have lung cancer, but their treatment plans may differ if one cancer has an actionable mutation and the other does not.
However, precision oncology does not mean that every patient will find a target, receive tablets instead of chemotherapy or avoid side effects. It is a decision-support approach, not a guarantee of response.
How is the decision made in real oncology practice?
In real practice, the decision begins with the basics. The diagnosis must be confirmed, the stage must be understood and the pathology report must be reviewed carefully.
Only after that does the oncologist decide whether biomarker testing, immunohistochemistry, FISH, PCR, NGS, liquid biopsy or germline genetic testing is needed.
The choice of test depends on the cancer type, available tissue, urgency of treatment, prior treatment history, cost, expected clinical benefit and whether the result will change management.
For example, in advanced non-small cell lung cancer, molecular testing may be important before finalising first-line systemic therapy. In some early-stage cancers, the role of molecular testing may be more selective and dependent on pathology, recurrence risk or treatment planning.
A careful oncologist does not order every possible test for every patient. The aim is to order the right test at the right time, using the right sample, for the right clinical question.
What reports and tests are usually required before deciding?
Before precision oncology can be interpreted properly, the oncologist usually needs the full clinical picture. A molecular report without context can be misleading.
The most useful documents usually include the biopsy report, immunohistochemistry report, imaging reports, stage details, treatment history, surgery notes if available and previous chemotherapy, immunotherapy or targeted therapy records.
Depending on the cancer type, the oncologist may request one or more of the following:
- Histopathology report confirming the cancer type
- Immunohistochemistry markers relevant to the diagnosis
- CT, PET-CT, MRI or other staging scans
- Biomarker testing such as ER, PR, HER2, PD-L1, MMR or MSI where relevant
- Next-generation sequencing, also called NGS, in selected cancers
- Liquid biopsy when tissue is inadequate or repeat biopsy is difficult
- Germline genetic testing when hereditary cancer risk is suspected
- Baseline blood tests and organ function assessment before treatment
The important point is that precision oncology is not based on one report alone. It requires integration of pathology, molecular data and clinical judgment.
What are the common mistakes patients should avoid?
One common mistake is assuming that NGS is always necessary before every cancer treatment. It is useful in many situations, but not universally required.
Another mistake is starting treatment before essential biomarkers are available, especially in cancers where first-line treatment can change based on biomarker results.
Some patients also interpret every mutation as “actionable.” A mutation may be present, but it may not have an approved treatment, may not be relevant in that cancer type or may only suggest a clinical trial.
Another concern is testing without enough tissue planning. If a small biopsy is exhausted by repeated small tests, there may not be enough material left for a broader panel later.
Cost is also important in the Indian clinical setting. The test should be chosen after discussing expected benefit, urgency, affordability and whether the result is likely to change treatment.
When should precision oncology be discussed before treatment starts?
Precision oncology should be discussed early when the cancer type has established treatment-relevant biomarkers. This is particularly important in advanced cancers where targeted therapy or immunotherapy may be considered.
It should also be discussed in recurrent cancer, rare cancers, young patients with unusual cancer patterns, strong family history of cancer and situations where standard treatment options are limited.
In elderly patients, precision oncology must be balanced with fitness, organ function, frailty, comorbidities and treatment tolerance. In young adults, fertility, long-term side effects, family risk and survivorship concerns may also influence decisions.
The timing matters. If molecular results are likely to change the first treatment, testing should ideally be planned before starting systemic therapy, unless treatment cannot safely wait.
Precision oncology decision tree: how should patients think about the next step?
If → Then decision logic:
- If cancer is newly diagnosed → Then first confirm the diagnosis, stage and pathology before finalising treatment.
- If the cancer type commonly requires biomarkers → Then ask whether biomarker testing should be completed before starting systemic therapy.
- If tissue is limited → Then discuss whether tissue should be preserved for NGS, whether repeat biopsy is needed or whether liquid biopsy is appropriate.
- If NGS shows an alteration → Then clarify whether it is actionable, approved in that cancer type, trial-relevant or only of uncertain significance.
- If treatment options are expensive or have major side effects → Then review expected benefit, alternatives, toxicity, logistics and affordability.
- If reports are incomplete or opinions differ → Then a structured cancer second opinion can help review diagnosis, stage, biomarkers and treatment sequence.
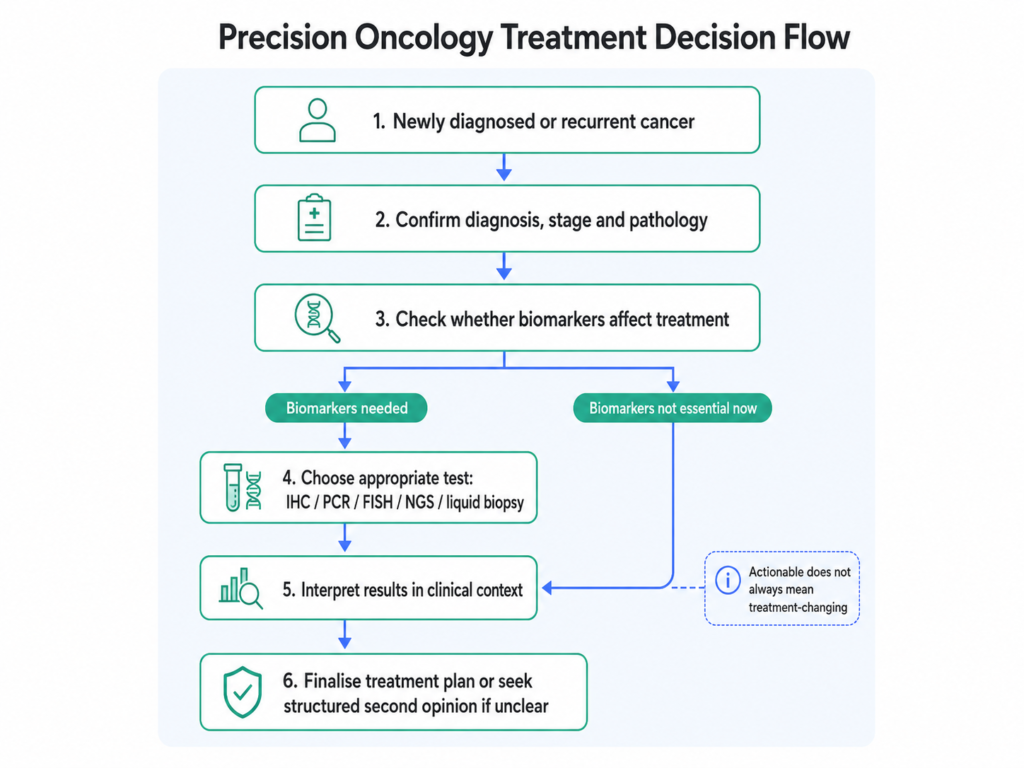
Precision oncology helps oncologists integrate diagnosis, stage, biomarkers and molecular profiling into cancer treatment planning
When should a second opinion be considered in precision oncology?
A second opinion is not about doubting the treating team. It is often useful when the diagnosis, stage, biomarker status or treatment sequence needs careful review.
Precision oncology can involve complex reports with technical terms such as variants, fusions, amplifications, tumour mutational burden, microsatellite instability and variants of uncertain significance. These results must be interpreted in relation to the patient’s cancer type and treatment goal.
A structured second opinion may be helpful when treatment is high-cost, when targeted therapy or immunotherapy is being considered, when cancer has recurred, when reports appear incomplete or when different doctors have suggested different approaches.
It can also help patients understand whether more testing is genuinely needed, whether an existing test is sufficient and whether a molecular tumour board discussion may add value.
What patients should clarify with their oncologist
Before making treatment decisions, patients and caregivers can use this practical checklist during consultation.
- Has the cancer diagnosis and subtype been confirmed by pathology?
- What is the stage of cancer, and is the treatment goal curative, disease-control or symptom-focused?
- Are any biomarkers essential before starting treatment?
- Is NGS needed, or is a smaller single-gene or limited biomarker test enough?
- Is there adequate tissue for molecular testing?
- Would liquid biopsy be useful if tissue is not available?
- If a mutation is found, is it clearly actionable in this cancer type?
- How will the test result change chemotherapy, targeted therapy, immunotherapy or follow-up decisions?
Frequently asked questions about precision oncology cancer treatment
Who should consider precision oncology in cancer treatment?
Patients with advanced cancer, recurrent cancer, rare cancers or cancers where biomarkers guide treatment should discuss precision oncology with their oncologist. It may also be relevant for younger patients, patients with strong family history or those considering targeted therapy or immunotherapy.
Is precision oncology the same as NGS testing?
No. NGS is one tool used in precision oncology. Precision oncology also includes pathology review, staging, biomarker testing, genetic counselling, treatment planning, patient fitness assessment and interpretation of results in clinical context.
Does precision oncology mean I will not need chemotherapy?
Not always. Some patients may receive targeted therapy or immunotherapy based on biomarkers, but others may still need chemotherapy, surgery, radiation or a combination. Precision oncology helps choose treatment more carefully; it does not automatically remove the need for chemotherapy.
What information is needed before deciding on molecular testing?
The oncologist usually needs the biopsy report, cancer subtype, stage, imaging results, prior treatment history, tissue availability and the clinical question being asked. Testing is most useful when the result can change treatment decisions.
When should an oncologist review a precision oncology report?
An oncologist should review the report before treatment decisions are made, especially if the report includes actionable mutations, uncertain variants, immunotherapy markers or possible hereditary cancer findings.
Can precision oncology help in cancer recurrence?
Yes, in selected cases. In recurrent cancer, repeat biopsy, biomarker reassessment or molecular profiling may help identify resistance mechanisms, new treatment options or clinical trial possibilities. The decision depends on the cancer type, previous treatment and current condition.
Related articles
- When Should Cancer Patients Consider Genetic or Molecular Testing?
- NGS Test in Cancer: When Is It Needed and What Does It Tell You?
- NGS vs Single-Gene Testing in Cancer: Which Test Should You Choose?
- When Should You Take a Cancer Second Opinion?
- Precision Oncology in India: What Patients and Doctors Should Know
Closing perspective
Precision oncology is not about replacing clinical judgment with a test report. It is about combining pathology, stage, biomarkers, molecular information and patient-specific factors to make cancer treatment decisions more thoughtful.
For patients and families, the goal is to ask better questions before starting treatment. For referring doctors, the goal is to identify when timely biomarker testing or oncology referral can prevent delays and improve decision quality.
The most useful precision oncology discussion is practical: What is the diagnosis? What is the stage? Which biomarkers matter? What test is appropriate? And how will the result change treatment?
Educational disclaimer: This article is for educational purposes only and does not replace personalised medical advice. Cancer treatment decisions should be made after reviewing the patient’s diagnosis, stage, pathology, biomarkers, fitness, preferences and overall clinical context with a qualified oncology team.
Related links
When and Why Genetic Testing Matters in Cancer Treatment and Prevention ?
How Molecular Profiling Influences Treatment Decisions in Lung Cancer