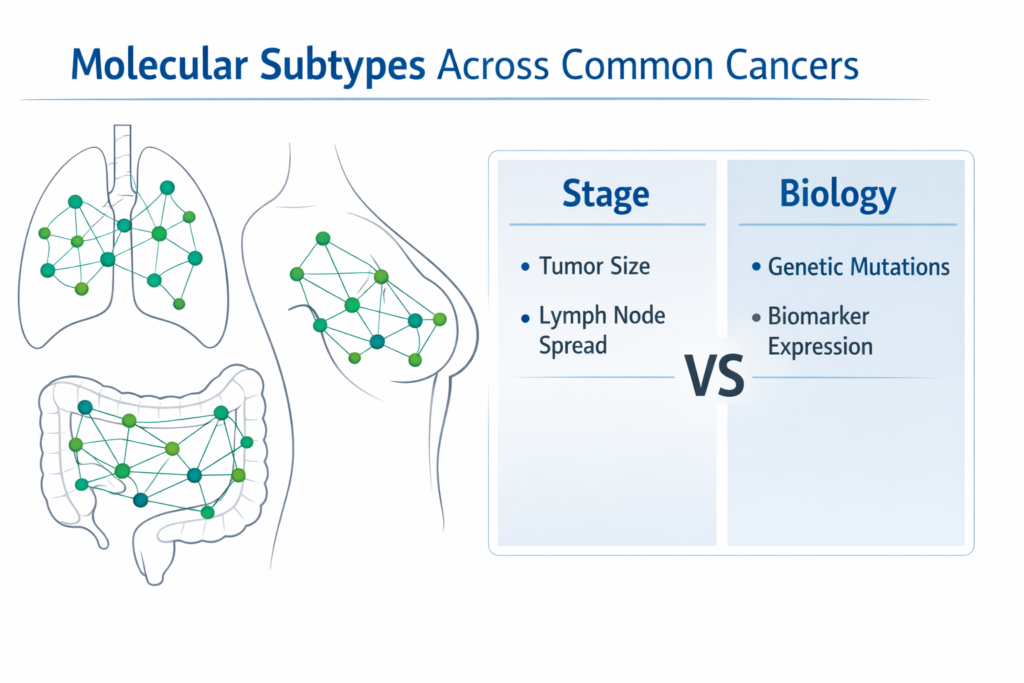
Cancer stage describes where the disease has spread. Molecular subtypes in cancer explains how the cancer behaves. In modern oncology, treatment decisions increasingly depend on tumor biology rather than anatomy alone. Two patients with the same stage may require entirely different therapies based on genetic drivers and biomarker expression.
As a medical oncologist working extensively in precision-driven treatment planning, I have observed that biology often predicts response, resistance, and survival more accurately than stage alone.
What Does “Molecular Subtype” Actually Mean?
A molecular subtype refers to the specific genetic mutations, receptor expressions, or signaling pathways driving tumor growth.
- Breast cancer: ER/PR positive, HER2 amplified, Triple-negative
- Lung cancer: EGFR, ALK, KRAS, BRAF mutations
- Colorectal cancer: MSI-high, KRAS mutant, BRAF mutant
- Melanoma: BRAF V600E mutation
These biological differences directly influence drug selection, toxicity expectations, and long-term prognosis.
Why Can Two Stage II Cancers Behave Completely Differently?
Stage measures tumor size and nodal involvement. It does not measure cellular aggression or molecular signaling.
- A Stage II HER2-positive breast cancer may respond dramatically to targeted therapy.
- A Stage II triple-negative breast cancer may require aggressive chemotherapy.
- A Stage IV EGFR-mutant lung cancer may respond better than Stage II KRAS-mutant disease.
In multiple cancers, molecular drivers can outweigh anatomical staging in therapeutic planning.
How Does Biology Change Treatment Strategy?
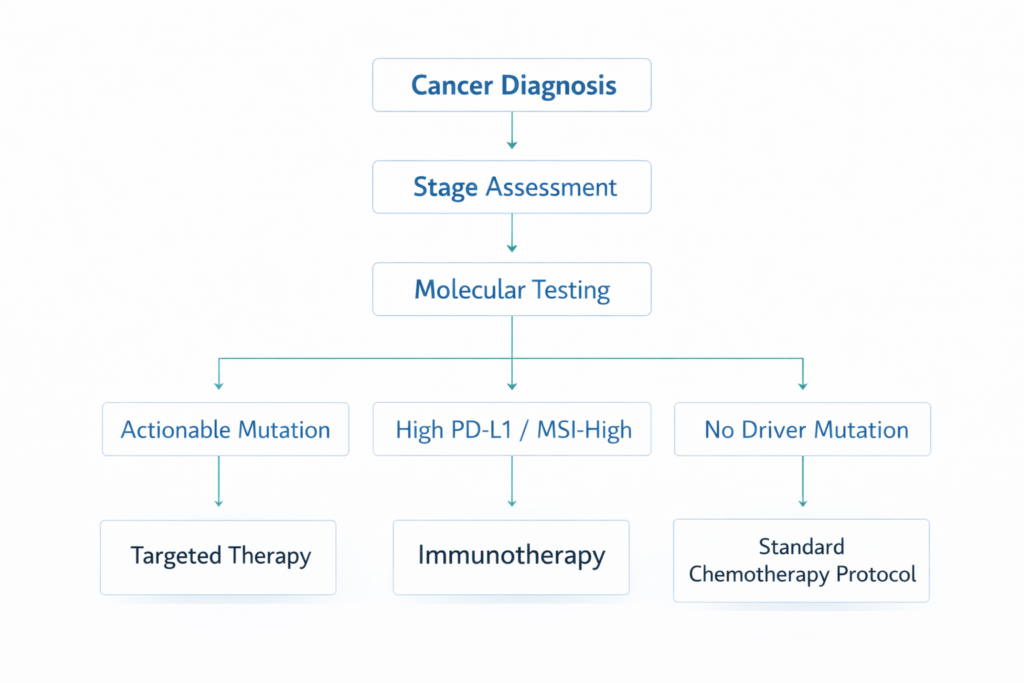
Modern oncology follows structured biomarker-driven logic.
- If actionable mutation → Targeted therapy
- If high PD-L1 expression → Immunotherapy ± chemotherapy
- If MSI-high → Immunotherapy preferred
- If hormone receptor positive → Endocrine therapy backbone
- If no driver mutation → Standard chemotherapy protocol
This approach personalizes intensity, sequence, and combination of therapy.
Structured Decision Logic: Stage vs Biology
Step 1: Confirm anatomical stage.
Step 2: Perform comprehensive molecular testing.
Step 3: Apply treatment logic:
- If early stage + high-risk mutation → Escalate systemic therapy.
- If advanced stage + strong actionable mutation → Consider targeted monotherapy.
- If low-risk biology despite nodal involvement → Avoid overtreatment.
- If no actionable marker → Follow evidence-based stage protocol.
This framework prevents both undertreatment and unnecessary toxicity.
When Should a Second Opinion Focus on Molecular Review?
A structured second opinion becomes crucial when:
- Comprehensive genomic testing was not performed.
- Treatment plan does not align with biomarker status.
- Rare mutations are detected.
- Disease progression occurs unexpectedly.
Precision oncology requires alignment between pathology, imaging, and molecular data.
Frequently Asked Questions
Is stage still important in cancer care?
Yes. Stage guides surgical planning and baseline prognosis, but biology refines systemic therapy decisions.
Do all cancers require molecular testing?
Not all. However, lung, breast, colorectal, melanoma, and several others routinely require biomarker evaluation.
Can molecular subtype change over time?
Yes. Tumor evolution and treatment pressure may alter mutation profiles, necessitating repeat testing.
Does targeted therapy replace chemotherapy?
In selected subtypes, yes. In others, it complements or follows chemotherapy.
Why do outcomes differ in patients with similar stage?
Underlying genetic drivers influence growth rate, immune response, and drug sensitivity.
Closing Perspective
Modern oncology is transitioning from stage-based algorithms to biology-driven frameworks. The future of cancer care lies in understanding the molecular narrative behind each tumor. Structured interpretation of this data allows safer, smarter, and more individualized therapy.
Educational Disclaimer: This article is intended for educational purposes only and does not substitute personalized medical advice. Treatment decisions must be individualized after clinical consultation.
Related Reads
What Is Biomarker-Driven Therapy in Modern Oncology?
The Role of PD-L1 Testing Before Starting Immunotherapy
Molecular Subtypes of Breast Cancer and Their Treatment Implications